In completed clinical trials with DAYVIGO , there was no clear evidence for physical dependence or withdrawal symptoms with the prolonged use of DAYVIGO as assessed by the Tyrer Benzodiazepine Withdrawal Symptom Questionnaire.
Rebound insomnia was assessed following discontinuation of DAYVIGO relative to placebo and baseline in both elderly and non-elderly adult patients receiving DAYVIGO 5 mg or 10 mg after 1 month and 1 year. No statistically significant effects were seen on measures of sleep onset latency or time awake after sleep onset in comparison to baseline values or relative to placebo.
In a human abuse liability study conducted in recreational sedative users (N=39), DAYVIGO (10, 20, and 30 mg) produced similar responses on positive subjective measures such as “Drug Liking”, “Overall Drug Liking”, “Take Drug Again”, and “Good Drug Effects” as zolpidem (30 mg) and suvorexant (40 mg), which were statistically significantly greater than placebo. Because individuals with a history of abuse or addiction to alcohol or other drugs may be at increased risk for abuse and addiction to DAYVIGO , follow such patients carefully.
In a 6-month, global, multicentre, randomized, double-blind, parallel-group phase III study, a similar incidence of adverse events was observed across the placebo, DAYVIGO 5 mg, and DAYVIGO 10 mg treatment groups.

Postural Stability
In 2 randomized, placebo- and active-controlled trials in healthy subjects and patients with insomnia ≥55 years of age:
No meaningful differences were observed between DAYVIGO (5 mg or 10 mg) and placebo2

Driving
In a randomized, double-blind, placebo, 4-period crossover study of healthy volunteers (N=48):
DAYVIGO at doses of 5 mg and 10 mg did not cause statistically significant impairment in next-morning driving performance in adult or elderly subjects (compared with placebo). However, driving ability was impaired in some subjects taking 10 mg DAYVIGO . Therefore, patients using the 10 mg dose should be cautioned about the potential for next-morning driving impairment3.

Cognitive Performance
In 2 randomized placebo trials in healthy subjects and insomnia patients ≥55 years of age:
There was no difference between DAYVIGO (5 mg or 10 mg) and placebo in test of memory2.

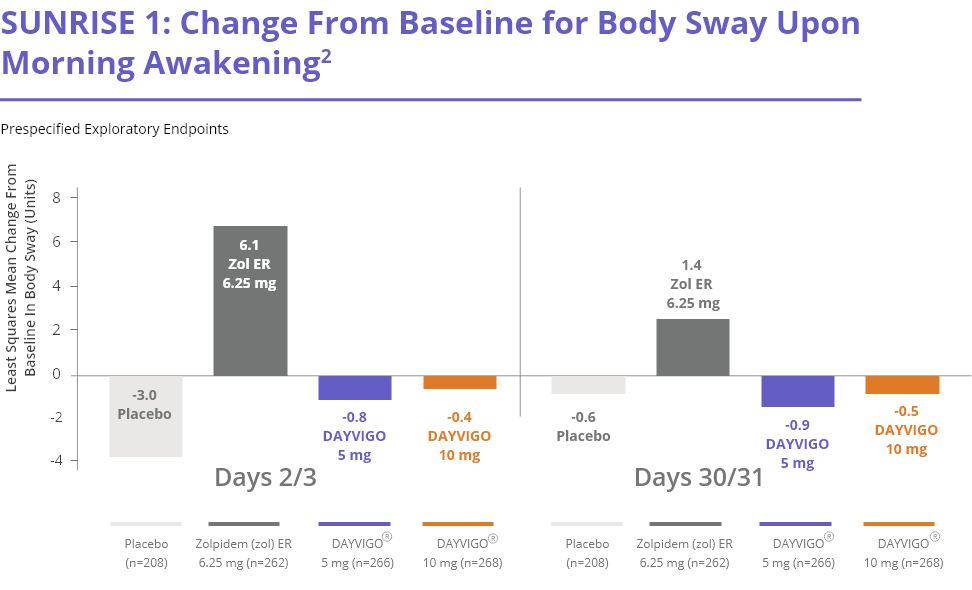
Postural Stability
Both DAYVIGO doses (5 mg and 10 mg) impaired balance (measured by body sway) at 4 hours post-dose compared with placebo2.
However, higher body sway was noted with subjects on Zolpidem therapy, which was statistically significant versus both doses of Dayvigo

Memory
Dayvigo 5 mg dosage showed comparable data to the Placebo arm on all the 4 domains which were tested for attention & memory after waking up the subjects around 4 hours of bed-time. Additionally, Dayvigo 5 mg dosage showed statistically significant data compared to Zolpidem group in 3 out of 4 domains of Cognition tested. However, caution has to be noted in some patients on 5 mg & patients on 10 mg dosage of Dayvigo with regards to Middle of the Night Cognitive Impairment.

Awakening to sound
Neither DAYVIGO dose demonstrated any meaningful differences in patients’ ability to awaken to sound compared with placebo2.
There was no difference between DAYVIGO (5 mg or 10 mg) and placebo in test of memory2.
DAYVIGO was generally well tolerated
Percentage of Patients with Treatment-Emergent Adverse Events (Incidence ≥ 1% in any DAYVIGO treatment group where the incidence in the DAYVIGO group was more than placebo from SUNRISE 1 and SUNRISE 2.)
| Placebo | DAYVIGO | |||
|---|---|---|---|---|
| N=528(%) | 5 Mg N=580(%) |
10 Mg N=582(%) |
||
| Gastrointinal Disorders | Nausea | 0.2 | 1.4 | 0.7 |
| General Disorders & Administration Site | Fatigue | 0 | 2.9 | 1.5 |
| Infections & Infestations | Nasopharyngitis | 0.9 | 2.8 | 1.7 |
| Upper Respiratory Tract Infection | 0.9 | 1.2 | 0.7 | |
| Urinary Tract Infections | 1.1 | 0.7 | 2.1 | |
| Muskuloskeletal & Connective Disoreders | 0.6 | 0.7 | 1.0 | |
| Nervous System Disorders | Headache | 4.0 | 6.0 | 4.6 |
| Somnolence | 1.3 | 5.5 | 8.4 | |
| Psychiatric Disorders | Abnormal Dreams | 0.8 | 0.3 | 1.0 |
| Nightmare | 0.4 | 0.5 | 1.0 | |
Sleep Paralysis
Sleep paralysis, an inability to move or speak for up to several minutes during sleep-wake transitions, can occur with the use of DAYVIGO . In clinical trials of DAYVIGO , sleep paralysis was reported: DAYVIGO 5 mg 1.3% or DAYVIGO 10 mg 1.6% compared to no reports for placebo (see WARNINGS AND PRECAUTIONS).
Hypnagogic Hallucinations
Hypnagogic hallucinations were reported in 0.1% and 0.7% of patients receiving DAYVIGO 5 mg and 10 mg, respectively, compared to no reports for placebo (see WARNINGS AND PRECAUTIONS).
Complex Sleep Behaviours
Two events of complex sleep behaviour were reported, both in patients receiving DAYVIGO 10 mg (see WARNINGS AND PRECAUTIONS).
Seizure
One subject in clinical trials receiving DAYVIGO 25 mg experienced two events of seizure approximately 2 hours and 3.5 hours after taking study medication on the same evening. The subject had no prior history of seizure disorder, though it is not clear that the episodes experienced had a causal relationship to DAYVIGO .
DAYVIGO should not be prescribed concomitantly with:
Avoid concomitant use of DAYVIGO with moderate or strong CYP3A inducers or inhibitors. The maximum recommended dose of DAYVIGO is 5 mg, no more than once per night when co-administered with weak CYP3A inducers and inhibitors.