
DAYVIGO was assessed vs placebo across 2 pivotal trials including nearly 2000 adult patients. Studies measured sleep onset and maintenance at Month 1 (sleep labs) and Month 6 (patient diaries).
At the proven starting dose of 5 mg, and at 10 mg, DAYVIGO was demonstrated superior to placebo across 2 pivotal trials.
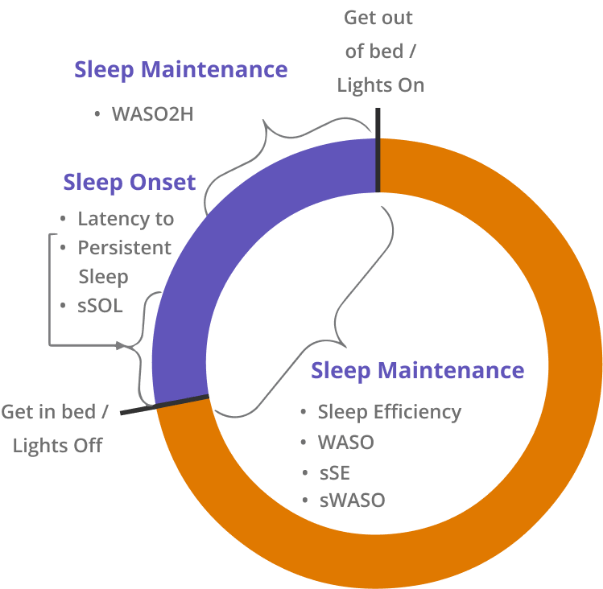
minutes from lights off to the first epoch of 20 consecutive (30-second) epochs of non-wakefulness
proportion of time spent asleep per Time in Bed (TIB), calculated as Total Sleep Time (TST)/interval from lights off until lights on
minutes of wake from the onset of persistent sleep until lights on
minutes of wake during the interval from 240 minutes after lights off until lights on
estimated minutes from the time that the subject attempted to sleep until sleep onset
pproportion of subjective total sleep time per subjective time spent in bed
sum of estimated minutes of wake during the night after initial sleep onset until the time the subject stopped trying to sleep for the night, operationalized as the time the subject got out of bed for the day
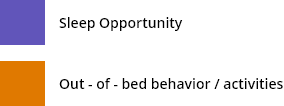
DAYVIGO reduced time to sleep onset, as assessed by the primary endpoint (mean* change from baseline in LPS vs placebo at Month 1).
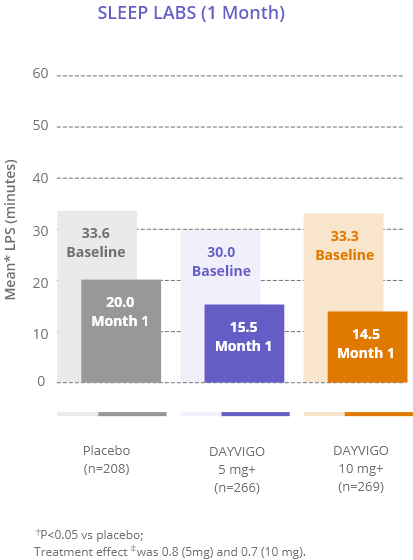
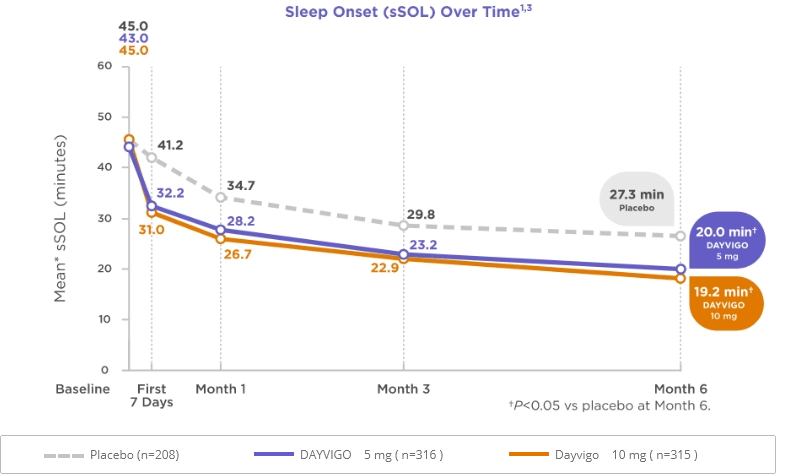
DAYVIGO reduced time to sleep onset, asassessed by the primary endpoint (mean* change from baseline in sSOL vs placebo at Month 6).
LPS=latency to persistent sleep; sSOL=subjective sleep onset latency.
* For the sleep onset endpoints (LPS, sSOL), the mean refers to least squares geometric mean, which was used due to the approximately log normal distribution of the outcomes.
‡ Treatment effect refers to the ratio of [Day 29/30 LPS / Baseline LPS] or [Month 6 sSOL / Baseline sSOL] for DAYVIGO vs placebo, such that a smaller ratio corresponds to a greater improvement.

Key primary endpoint: Mean* change from baseline in LPS at Month 1 for DAYVIGO 5 mg and 10 mg compared to placebo.
Prespecified exploratory endpoints: Mean* change from baseline in LPS at Month 1 for DAYVIGO 5 mg and 10 mg compared to zolpidem ER. Mean* change from baseline in LPS at Day 1/2 for DAYVIGO 5 mg and 10 mg compared to placebo and zolpidem ER.
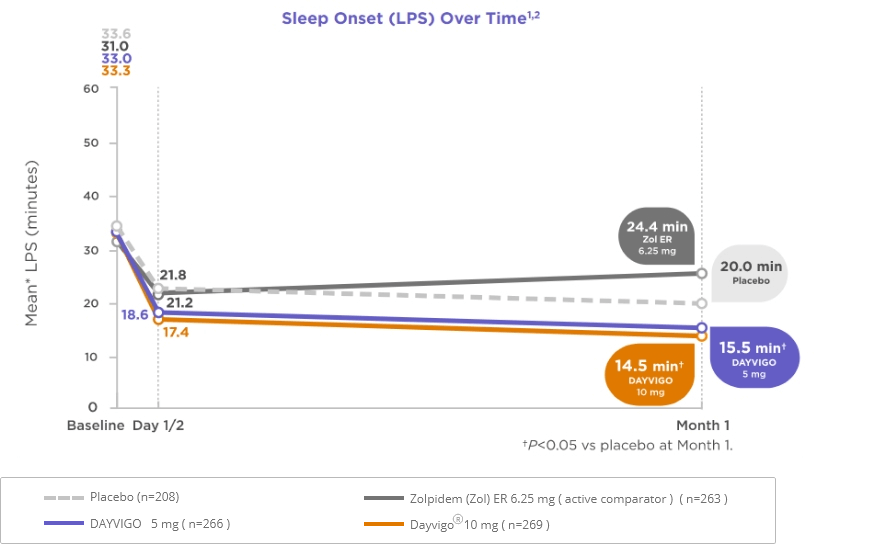
ER=extended release;
Limitations:Prespecified exploratory endpoints were not adjusted for multiplicity and were not adequately powered to show statistical significance. These data are not intended to imply the superiority of DAYVIGO vs zolpidem ER.

Key primary endpoint: Mean* change from baseline in LPS at Month 1 for DAYVIGO 5 mg and 10 mg compared to placebo.
Prespecified exploratory endpoints: Mean* change from baseline in LPS at Month 1 for DAYVIGO 5 mg and 10 mg compared to zolpidem ER. Mean* change from baseline in LPS at Day 1/2 for DAYVIGO 5 mg and 10 mg compared to placebo and zolpidem ER.
Limitations:Prespecified exploratory endpoints were not adjusted for multiplicity and were not adequately powered to show statistical significance.
LPS=latency to persistent sleep; sSOL=subjective sleep onset latency.
* For the sleep onset endpoints (LPS, sSOL), the mean refers to least squares geometric mean, which was used due to the approximately log normal distribution of the outcomes.
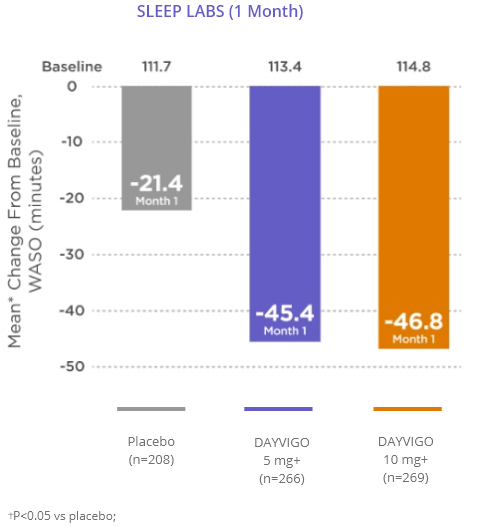
DAYVIGO reduced WASO, as assessed by the secondary endpoint (mean* change from baseline in WASO vs placebo at Month 1).
DAYVIGO reduced sWASO, as assessed by the secondary endpoint (mean* change from baseline in sWASO vs placebo at Month 6).
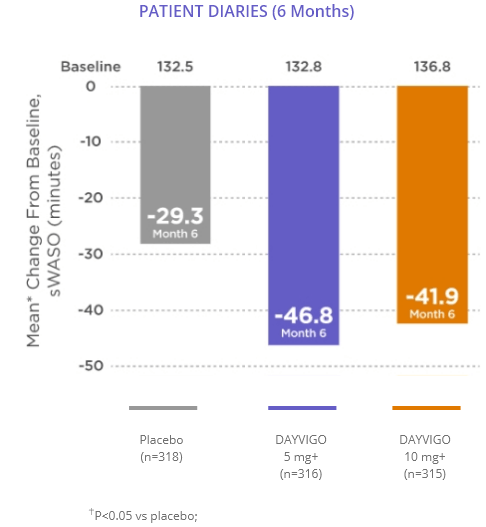
sWASO=subjective wake after sleep onset; WASO=wake after sleep onset.
* For sleep maintenance endpoints (WASO, sWASO), the mean refers to least squares mean.
Key secondary endpoint: Mean change from baseline in WASO at Month 1 for DAYVIGO 5 mg and 10 mg compared to placebo.
Prespecified exploratory endpoints: Mean change from baseline in WASO at Month 1 for DAYVIGO vs zolpidem ER. Mean change from baseline in WASO at Day 1/2 for DAYVIGO vs placebo and zolpidem ER.
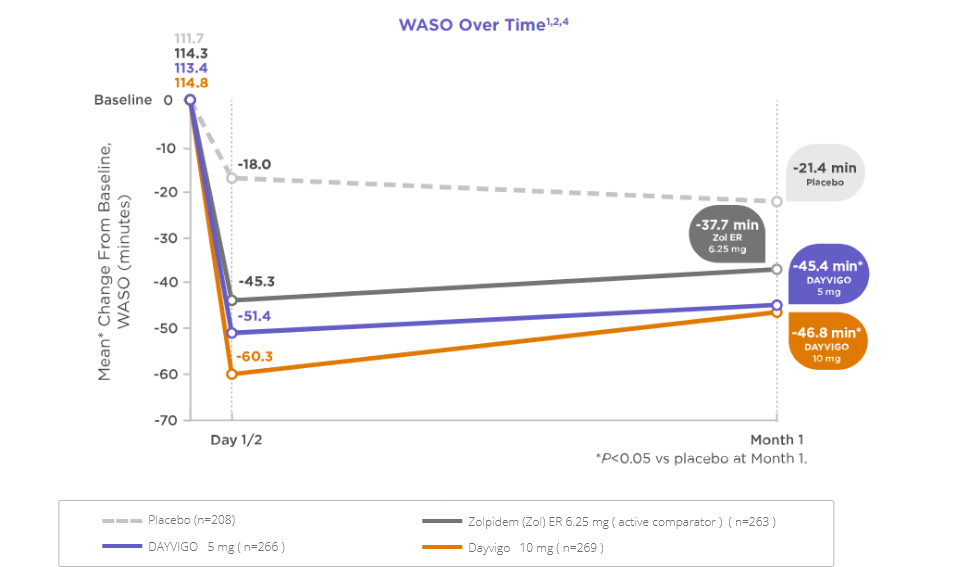
ER=extended release;
Limitations:Prespecified exploratory endpoints were not adjusted for multiplicity and were not adequately powered to show statistical significance. These data are not intended to imply the superiority of DAYVIGO vs zolpidem ER.
Key primary endpoint: Mean change from baseline in sWASO at Month 6 for DAYVIGO 5 mg and 10 mg compared to placebo.
Prespecified exploratory endpoints: Mean change from baseline in sWASO at First 7 Days, Month 1, and Month 3 for DAYVIGO vs placebo.
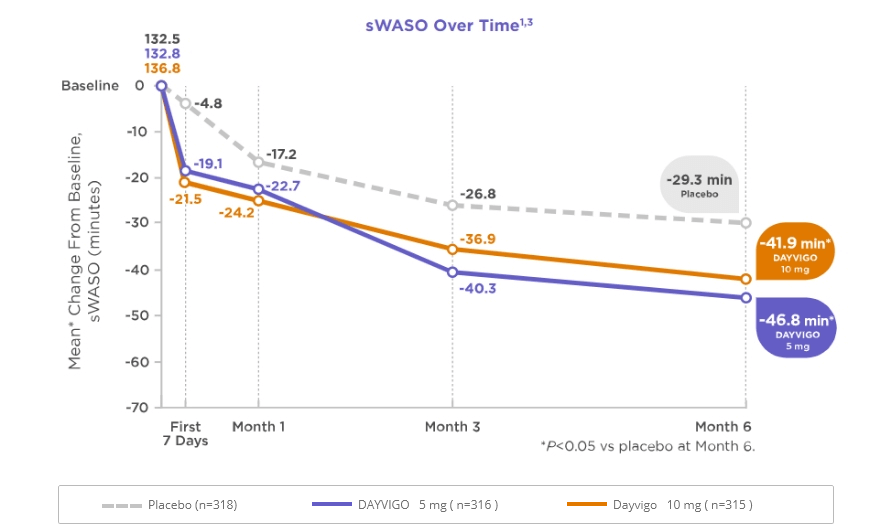
Limitations:Prespecified exploratory endpoints were not adjusted for multiplicity and were not adequately powered to show statistical significance.
ER=extended release; sWASO=subjective wake after sleep onset; WASO=wake after sleep onset.
* For sleep maintenance endpoints (WASO, sWASO), the mean refers to least squares mean.
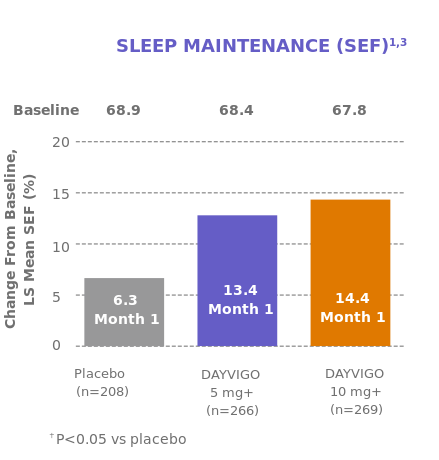
DAYVIGO increased SEF, as assessed by the secondary endpoint (mean* change from baseline in SEF vs placebo at Month 1).
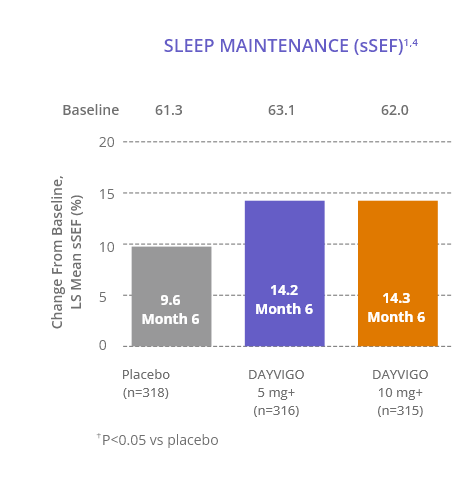
DAYVIGO increased sSEF, as assessed by the secondary endpoint (mean* change from baseline in sSEF vs placebo at Month 6).
SEF=sleep efficiency; sSEF=subjective sleep efficiency.
SEF=sleep efficiency; sSEF=subjective sleep efficiency.
Key secondary endpoint: Mean change from baseline in SEF at Month 1 for DAYVIGO 5 mg and 10 mg compared to placebo.
Prespecified exploratory endpoints: Mean change from baseline in SEF at Month 1 for DAYVIGO vs Zolpidem ER. Mean change from baseline in SEF at Day 1/2 for DAYVIGO vs placebo and zolpidem ER.
Limitations:Prespecified exploratory endpoints were not adjusted for multiplicity and were not adequately powered to show statistical significance. These data were not intended to imply the superiority of DAYVIGO vs Zolpidem ER.
Key primary endpoint: Mean change from baseline in sSEF at Month 6 for DAYVIGO 5 mg and 10 mg compared to placebo.
Prespecified exploratory endpoints: Mean change from baseline in sSEF to First 7 Days, Month 1, and Month 3 for DAYVIGO vs placebo.
Limitations:Prespecified exploratory endpoints were not adjusted for multiplicity and were not adequately powered to show statistical significance.
ER=extended release; SEF=sleep efficiency; sSEF=subjective sleep efficiency.
* For sleep maintenance endpoints (SEF, sSEF), the mean refers to least squares mean.
Prespecified exploratory endpoints: Mean change from baseline in sSEF to First 7 Days, Month 1, and Month 3 for DAYVIGO vs placebo.
The initial 6-month placebo-controlled treatment period was followed by a 6-month parallel-group extension period.
At the start of the extension period, patients taking DAYVIGO in the 6-month placebo-controlled study continued on their previous dose of DAYVIGO during the 6-month parallel-group extension period. Patients on placebo during the 6-month placebo-controlled study were re-randomized to either DAYVIGO 5 mg or 10 mg.
sSEF Over Time6 (Placebo Patients Re-Randomized to DAYVIGO )
The placebo group during the 6-month placebo-controlled study re-randomized to DAYVIGO 5mg (n=128) and 10 mg (n=122) at the start of the extension period showed baseline sSEF values at Month 6 (0 months of DAYVIGO exposure) of 70.5% and 71.1%, respectively. The mean change from baseline, sSEF measures at Month 9 (3 months of DAYVIGO exposure) are 4.7% (5 mg), 5.1% (10 mg) and at Month 12 (6 months of DAYVIGO exposure) are 3.9% (5 mg) and 4.5% (10 mg).
Limitations:Prespecified exploratory endpoints were not adjusted for multiplicity and were not adequately powered to show statistical significance. Extension period did not include a placebo comparator and was therefore not designed to draw efficacy conclusions.5
Polysomnography (sleep labs)
Sleep diaries (patient reports)
N=1006
1-month treatment period
Treatment arms
DAYVIGO 5 mg
DAYVIGO 10 mg
Active comparator (zolpidem ER 6.25 mg) Placebo
Males ≥65 years of age
Females ≥55 years of age
Median age: 63.0 years
86.0% female
27.0% non-white
45.0% ≥65 years of age
Sleep diaries (patient reports)
N=971
6-month placebo-controlled treatment period with6-month parallel-group extension period
Treatment arms
DAYVIGO 5 mg
DAYVIGO 10 mg
Placebo
Adults ≥18 years of age
Median age: 55.0 years
68.0% female
28.5% non-white
28.0% ≥65 years of age
All patients received instructions consistent with principles of good sleep hygiene.
BMI=body mass index; DSM-5=Diagnostic and Statistical Manual of Mental Disorders, 5th Edition.